
Benign Paroxysmal Positional Vertigo (BPPV)
Have you ever felt like you were spinning? Located in the inner ear are calcium carbonate crystals called otoconia, commonly referred to as “ear rocks.” When otoconia are displaced, patients may complain of dizziness and a sensation of movement (vertigo), often spinning, typically associated with lying down, rolling over in bed, tilting the head back or bending forward with the head down. Other symptoms may include imbalance, nausea, fogginess and a general sense of not feeling well.
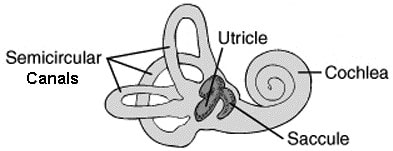
It is helpful to understand a little about the anatomy of the inner ear. There are 3 semicircular canals. Each canal starts and ends at the utricle. The utricle and saccule, which make up the vestibule, both contain otoconia (ear rocks). Sometimes otoconia fall out of the utricle and into a canal. When this happens, it is known as Benign Paroxysmal Positional Vertigo (BPPV). Misplaced otoconia can be due to illness, age related changes, ear infection, trauma, prolonged bed rest, activities that place the head in a head up or head down position (i.e. dental procedures, reaching for a high shelf, washing your hair, bending over to put your shoes on, pulling weeds), and sometimes for no known reason. Research also suggests a correlation between BPPV and osteoporosis as well as diabetes.
It is important to report specific symptoms to a medical professional experienced in treating vestibular disorders to rule out other possible and more serious causes of symptoms. One of the diagnostic tools used to confirm BPPV is called the Dix-Hallpike test, a positioning test designed to elicit rapid eye movement (nystagmus) and/or vertigo. The specific direction and duration of the nystagmus is the key to confirming if you have BPPV, which of 2 main forms of BPPV you may have (canalithiasis vs cupulolithiasis) and identifying which of the 6 canals (3 on each side) is/are the offending canal(s). There are additionally atypical forms of BPPV which can be more challenging to identify.
Infrared Video Frenzel goggles are extremely beneficial to aide in a correct diagnosis, necessary to rule out other causes and are very helpful to educate the patient about their specific condition. Some vestibular tests cannot be performed without goggles. Once the offending canal(s) is/are properly diagnosed, the patient is taken through a series of movements to maneuver the “ear rocks” back where they belong. There are many maneuvers depending on the type of BPPV, the involved canal(s), the patient’s presentation, and the skill and knowledge of the professional. When the correct maneuver is performed accurately, treatment is extremely successful, often resolving symptoms in 1-3 sessions.
Have you ever felt like you were spinning? Located in the inner ear are calcium carbonate crystals called otoconia, commonly referred to as “ear rocks.” When otoconia are displaced, patients may complain of dizziness and a sensation of movement (vertigo), often spinning, typically associated with lying down, rolling over in bed, tilting the head back or bending forward with the head down. Other symptoms may include imbalance, nausea, fogginess and a general sense of not feeling well.
It is helpful to understand a little about the anatomy of the inner ear. There are 3 semicircular canals. Each canal starts and ends at the utricle. The utricle and saccule, which make up the vestibule, both contain otoconia (ear rocks). Sometimes otoconia fall out of the utricle and into a canal. When this happens, it is known as Benign Paroxysmal Positional Vertigo (BPPV). Misplaced otoconia can be due to illness, age related changes, ear infection, trauma, prolonged bed rest, activities that place the head in a head up or head down position (i.e. dental procedures, reaching for a high shelf, washing your hair, bending over to put your shoes on, pulling weeds), and sometimes for no known reason. Research also suggests a correlation between BPPV and osteoporosis as well as diabetes.
It is important to report specific symptoms to a medical professional experienced in treating vestibular disorders to rule out other possible and more serious causes of symptoms. One of the diagnostic tools used to confirm BPPV is called the Dix-Hallpike test, a positioning test designed to elicit rapid eye movement (nystagmus) and/or vertigo. The specific direction and duration of the nystagmus is the key to confirming if you have BPPV, which of 2 main forms of BPPV you may have (canalithiasis vs cupulolithiasis) and identifying which of the 6 canals (3 on each side) is/are the offending canal(s). There are additionally atypical forms of BPPV which can be more challenging to identify.
Infrared Video Frenzel goggles are extremely beneficial to aide in a correct diagnosis, necessary to rule out other causes and are very helpful to educate the patient about their specific condition. Some vestibular tests cannot be performed without goggles. Once the offending canal(s) is/are properly diagnosed, the patient is taken through a series of movements to maneuver the “ear rocks” back where they belong. There are many maneuvers depending on the type of BPPV, the involved canal(s), the patient’s presentation, and the skill and knowledge of the professional. When the correct maneuver is performed accurately, treatment is extremely successful, often resolving symptoms in 1-3 sessions.